Chest wall tumours are abnormal growths that originate in or spread to the various components of the chest wall. This complex anatomical structure includes bones (ribs, sternum, vertebrae), cartilage, muscles, connective tissues, nerves, and skin. These tumours can be either benign (non-cancerous) or malignant (cancerous) and may present unique diagnostic and therapeutic challenges due to their location and proximity to vital organs. Understanding their diverse origins, characteristics, and management strategies is critical for effective patient care.
1. Anatomy of the Chest Wall: A Protective Framework
The chest wall forms the protective cage around the heart and lungs. It is composed of:
- Bones: 12 pairs of ribs, the sternum (breastbone), and the thoracic vertebrae.
- Cartilage: Costal cartilages that connect the ribs to the sternum.
- Muscles: Including intercostal muscles, pectoralis muscles, and serratus muscles.
- Connective Tissue: Fascia, ligaments, and tendons.
- Skin and Subcutaneous Tissue: The outermost layers. A tumour in any of these components can be classified as a chest wall tumour.
2. Primary vs. Secondary Chest Wall Tumours
Chest wall tumours are broadly categorized based on their origin:
- Primary Chest Wall Tumours: These tumours originate directly from the tissues of the chest wall itself. They can be benign or malignant.
- Benign Primary Tumours: These are more common and include conditions like osteochondromas, chondromas, fibrous dysplasia, and desmoid tumours. They generally grow slowly and do not spread.
- Malignant Primary Tumours: These are rarer but more serious. Examples include chondrosarcoma (arising from cartilage), osteosarcoma (from bone), Ewing’s sarcoma, and rhabdomyosarcoma (from muscle).
- Secondary (Metastatic) Chest Wall Tumours: These are more common than primary malignant tumours and occur when cancer from another part of the body spreads (metastasizes) to the chest wall. Common primary cancers that metastasize to the chest wall include lung cancer, breast cancer, kidney cancer, prostate cancer, and thyroid cancer.
3. Symptoms and Clinical Presentation
The symptoms of a chest wall tumour vary depending on its size, location, and whether it’s benign or malignant. Common signs include:
- A palpable mass or lump: Often the first and most common symptom, which may or may not be painful.
- Pain: Localized chest wall pain is very common, especially with malignant tumours. The pain can be persistent, sharp, aching, or worse with movement, breathing, or pressure.
- Swelling: Over the affected area.
- Tenderness: When touching the lump or surrounding area.
- Neurological symptoms: If the tumour presses on nerves, leading to numbness, tingling, or weakness in an arm or hand.
- Respiratory symptoms: Shortness of breath if the tumour is large and restricts lung expansion, or if it involves the pleura.
- Systemic symptoms: For malignant tumours, unexplained weight loss, fever, or fatigue may occur.
4. Diagnosis and Evaluation
A thorough diagnosis of a chest wall tumour is essential to determine its type and extent. The process often involves:
- Physical Examination: Assessing the lump, pain, and any associated symptoms.
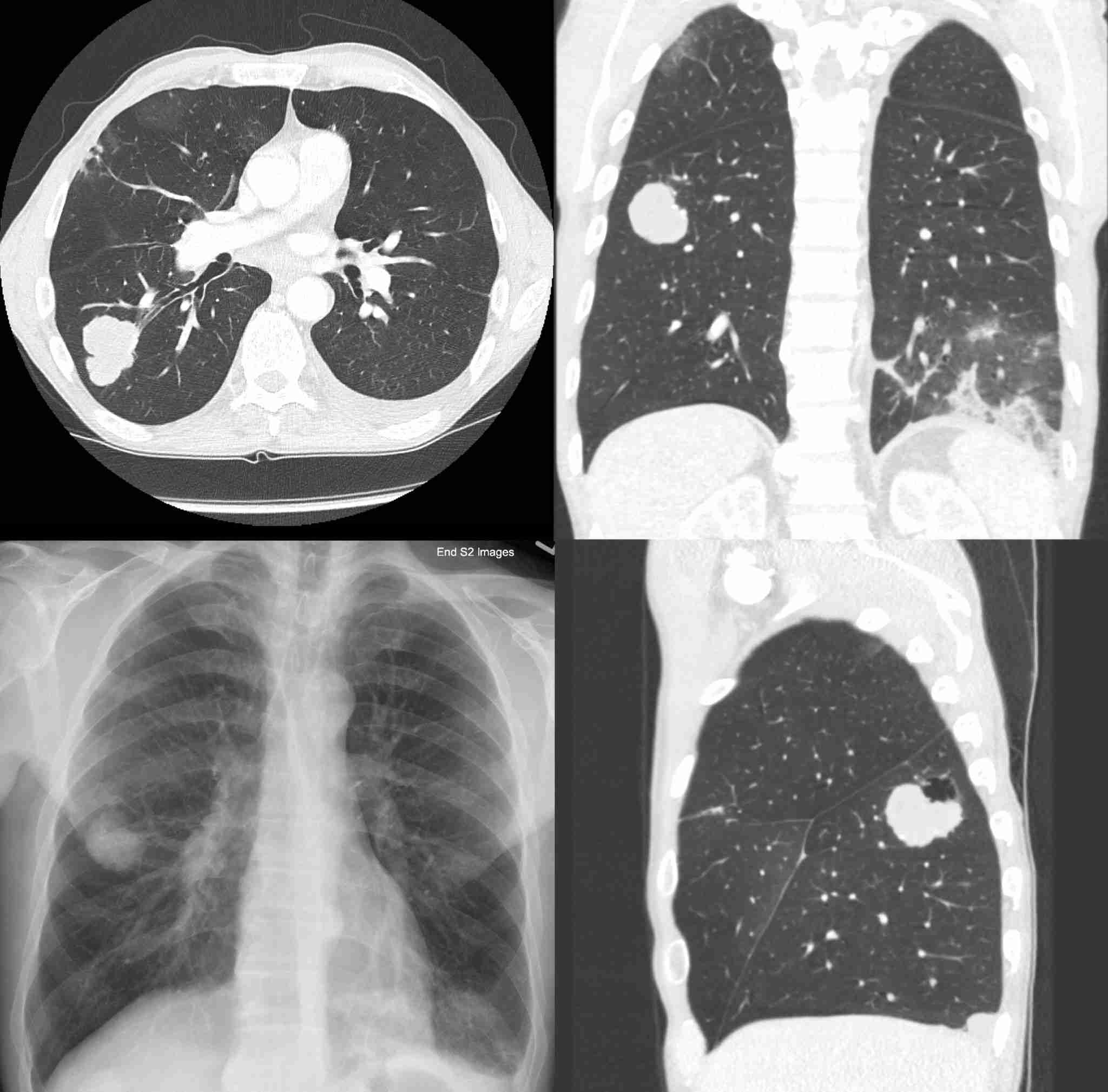
- Imaging Studies:
- X-rays: Initial imaging to identify bone involvement.
- Computed Tomography (CT) Scan: Provides detailed cross-sectional images of the chest wall, bones, and soft tissues.
- Magnetic Resonance Imaging (MRI): Excellent for visualizing soft tissue involvement, nerve compression, and tumour extent.
- Positron Emission Tomography (PET) Scan: Helps differentiate between benign and malignant lesions and detect distant metastases.
- Biopsy: This is crucial for definitive diagnosis. It involves taking a tissue sample from the tumour for pathological examination. Biopsy types include needle biopsy (core needle or fine-needle aspiration) or incisional/excisional surgical biopsy.
- Blood Tests: May be done to check general health or for specific tumour markers if cancer is suspected.
5. Treatment Options for Chest Wall Tumours
Treatment strategies for chest wall tumours are highly individualized and depend on whether the tumour is benign or malignant, its type, size, location, and the patient’s overall health. A multidisciplinary approach often involves thoracic surgeons, oncologists, radiation oncologists, and reconstructive surgeons.
- For Benign Tumours:
- Observation: Small, asymptomatic benign tumours may simply be monitored.
- Surgical Excision: Removal of the tumour is common if it causes symptoms, is growing, or if there’s any uncertainty about its benign nature.
- For Malignant Primary Tumours:
- Surgical Resection: This is often the primary treatment. It involves removing the tumour with a clear margin of healthy tissue, which may require removing ribs, sternum, or other parts of the chest wall. Extensive resections may necessitate reconstructive surgery using prosthetic materials or muscle flaps.
- Radiation Therapy: May be used before surgery (neoadjuvant) to shrink the tumour, after surgery (adjuvant) to kill any remaining cancer cells, or as a primary treatment if surgery is not feasible.
- Chemotherapy: Often used in conjunction with surgery and/or radiation, especially for sarcomas and other aggressive cancers.
- Targeted Therapy/Immunotherapy: Newer treatments that may be an option for specific types of malignant tumours.
- For Secondary (Metastatic) Tumours:
- Treatment focuses on managing the primary cancer. If the chest wall metastasis is isolated and resectable, surgery might be considered. Otherwise, systemic therapies like chemotherapy, radiation, or targeted therapy are used.
6. Prognosis and Rehabilitation
The prognosis for chest wall tumours varies significantly. Benign tumours generally have an excellent prognosis after removal. For malignant tumours, prognosis depends heavily on the type, stage, completeness of resection, and response to treatment. Post-operative rehabilitation is crucial, especially after extensive resections, to restore chest wall stability, lung function, and minimize pain. This may involve physical therapy, pain management, and respiratory exercises to help patients regain strength and function.